

After a record-breaking May Bank Holiday weekend in the UK, shorts, skirts and summer clothing appeared overnight. I found myself walking through town looking at a genuine cross-section of women’s legs of different ages, sizes and body shapes. Beautiful young girls, young and older women, all showed the same normal variations in cellulite, softer thighs, saddlebags and lower-body fat distribution. It did not look unusual or pathological. It looked like the normal spectrum of female bodies.
And it made me think again about the growing confusion surrounding cellulite or lipoedema, and how increasingly difficult many women now find it to know where normal female fat distribution ends and genuine disease begins.
What is Cellulite?
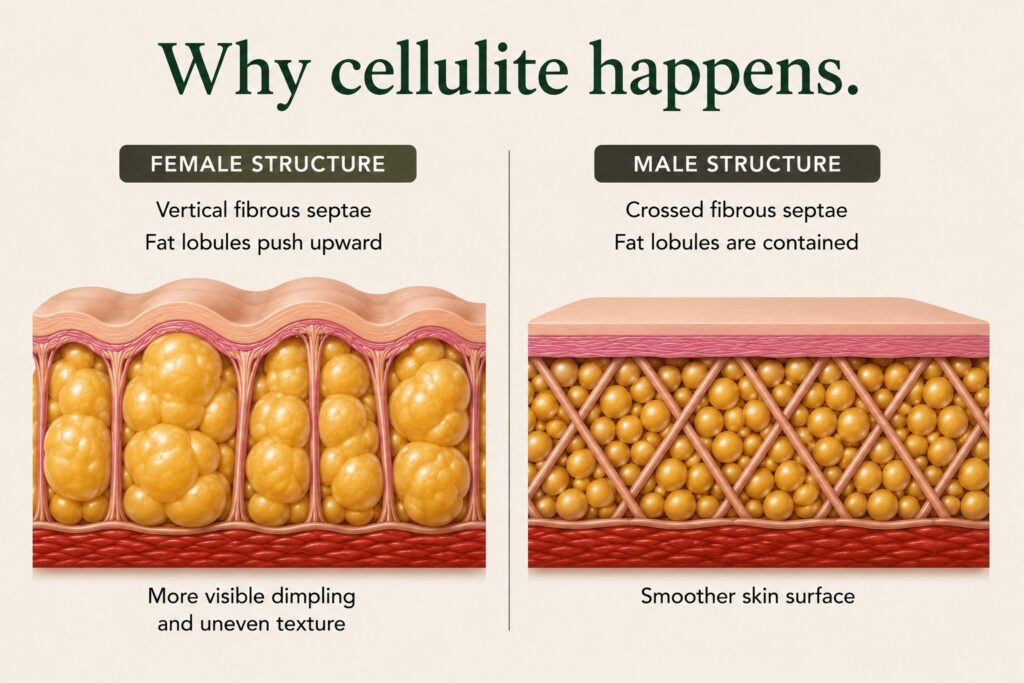
Cellulite is the term used to describe uneven, dimpled or rippled skin texture that most commonly develops around the hips, thighs and buttocks. It is caused by the way subcutaneous fat sits underneath the skin alongside fibrous connective tissue bands within the superficial fat layer.
Around 80–90% of post-pubescent women develop some degree of cellulite during their lifetime, compared with only around 5% of men.
In women, fibrous connective tissue bands (septae) within the superficial fat layer run vertically between the skin and deeper structures. Fat cells (adipocytes) can protrude upwards between these bands, producing visible dimpling and uneven skin texture.
Male connective tissue is arranged differently. The connective tissue underneath the skin forms a firmer cross-linked pattern, helping contain fat more evenly and making visible cellulite far less common in men.
This is why cellulite can occur in women who are otherwise extremely slim, fit and healthy. It is not simply a sign of obesity. It reflects female connective tissue structure itself.
Why Cellulite Commonly Develops Around the Lower Body
Women are biologically designed to store fat differently from men under the influence of female hormones. Fat distribution around the hips, thighs, buttocks and pelvis is closely linked to female reproductive physiology including menstruation, fertility, pregnancy and breastfeeding.
Many women first notice cellulite around puberty, when oestrogen begins altering fat distribution and body composition. Visible lower-body fat distribution and cellulite can therefore appear surprisingly early, even in slim healthy girls.
Ectomorphs, Mesomorphs and Endomorphs
Historically, people were often described as ectomorphs, mesomorphs or endomorphs. These categories described recognisable differences in body shape, fat distribution and physical performance.
Ectomorphs are typically tall, lean, long-limbed and straight up and down in shape, often with wiry figures and very little visible body fat. They are associated with fast metabolism, speed and explosive movement and often find it difficult to gain weight or store fat.
Mesomorphs are athletic in build, with broader shoulders, narrower waists and greater natural muscle development. They are generally viewed as physically balanced between strength, speed and endurance.
Endomorphs are pear-shaped, storing more fat around the hips, thighs and lower body. They are often heavier in build and more suited to endurance and sustained energy output than speed.
These descriptions reflected something people recognised instinctively for generations: women naturally differed in body shape and fat distribution. Fuller hips, cellulite and lower-body fat storage were not automatically viewed as abnormal or diseased.

So Where Does Lipoedema Fit Into This?
Lipoedema is a genuine chronic adipose tissue disease involving disproportionate fat accumulation, most commonly affecting the legs and sometimes the arms.
Unlike ordinary cellulite or constitutional lower-body fat distribution, lipoedema is usually associated with additional clinical features such as pain, tenderness, bruising, tissue heaviness, disproportion, multisystem dysregulation and progression over time. Hormonal onset or progression is also important, with many women reporting worsening symptoms around puberty, pregnancy or menopause.
However, the presence of cellulite alone is not enough to diagnose lipoedema. A woman can, and often does, have cellulite without having lipoedema. She can have softer thighs, saddlebags or a natural hormonally designed lower-body fat distribution without having disease.
Why Confusion Has Increased
Social media has increased awareness of lipoedema, which has helped many women who were previously dismissed or misunderstood. At the same time, cellulite, normal female fat distribution and genuine lipoedema are now often discussed as though they are interchangeable.
Women increasingly film themselves squeezing their thighs, pinching cellulite or showing normal lower-body fat distribution on social media while describing it as lipoedema.
They are not automatically the same thing. The danger is that ordinary female fat distribution increasingly becomes interpreted as evidence of hidden disease.
That is neither psychologically healthy nor medically accurate.
Can Liposuction Permanently Remove Cellulite?
Many women understandably hope that liposuction will permanently eliminate cellulite.
Body contour can sometimes improve it. However, liposuction does not fundamentally change female connective tissue structure. The original fibrous connective tissue arrangement underneath the skin still remains even after fat removal.
This helps explain why cellulite can be difficult to eliminate completely.
Understanding Why the Difference Matters
For women who genuinely have lipoedema, accurate diagnosis can be extremely important. It may help explain years of pain, heaviness, disproportion or failed attempts to manage tissue change through conventional dieting.
At the same time, it is equally important not to pathologise completely normal female anatomy.
Cellulite is extraordinarily common in women and, in many cases, simply reflects normal female connective tissue structure and female fat distribution rather than disease.
Awareness matters. Accurate assessment matters too.