


Lipoedema, Pain and Breathing Pattern Disorders
Many women who experience pain in lipoedema describe symptoms that extend beyond localised tissue pain. These may include fatigue, dizziness, palpitations, anxiety, gut disturbance, temperature sensitivity and poor sleep patterns. In some cases, women present with concurrent conditions such as Postural Orthostatic Tachycardia Syndrome (POTS) or fibromyalgia.
These symptoms can feel unrelated because they affect different body systems. However, they are often linked through how the nervous system regulates the body. Breathing is under autonomic control and may influence how these symptoms develop and persist, especially if a breathing pattern disorder is present.
What is the Autonomic Nervous System?
The autonomic nervous system regulates functions that happen automatically, without conscious thought, including heart rate, blood pressure, breathing, digestion, temperature control and sleep. It allows the body to respond to demand and return to a resting state.
When this system is not working efficiently, regulation becomes unstable. The body may remain in a heightened state or fluctuate between states, leading to symptoms such as palpitations, dizziness, fatigue, gut disturbance, temperature sensitivity and poor sleep. These patterns are commonly reported in women with lipoedema.
What Happens When We Breathe?
At rest, breathing is quiet and regular, typically 12–16 breaths per minute. It occurs through the nose, with the diaphragm controlling movement so the abdomen rises and falls gently.
When we inhale, oxygen is taken in for energy production. When we exhale, carbon dioxide (CO2) is released. Carbon dioxide is not simply a waste product. It plays an essential role in regulating blood chemistry, circulation and breathing.
What is a Breathing Pattern Disorder?
A breathing pattern disorder (BPD) occurs when normal breathing rhythm is lost and becomes inefficient. This may include upper chest breathing, rapid or shallow breathing (hyperventilation), mouth breathing, frequent sighing or yawning and increased use of the neck and shoulder muscles.
Over-breathing is a normal response to stress, pain or illness. However, it may persist after the original trigger has resolved and become habitual over time. This may develop in response to chronic pain, stress or anxiety, surgery or injury, or prolonged tension.
What Happens During Over-Breathing (Hyperventilation)?
When breathing becomes faster or deeper than the body requires, too much CO₂ is expelled from the lungs. This reduces the level of CO2 in the arterial blood supply, a state known as hypocapnia.
Carbon dioxide plays an essential role in maintaining normal blood pH. When CO2 levels fall, the blood becomes more alkaline, resulting in a mild respiratory alkalosis.
CO2↓ ⇒ pH↑
This change affects how oxygen is delivered to the tissues. As carbon dioxide falls and pH rises, the oxyhaemoglobin dissociation curve shifts to the left, meaning that haemoglobin holds on to oxygen more tightly and less is released to the tissues. As a result, even when oxygen levels in the blood are normal, delivery to working tissues may be reduced.
At the same time, low CO2 causes blood vessels to constrict, particularly in the brain and peripheral tissues, reducing blood flow. This can contribute to symptoms such as dizziness, light-headedness, fatigue and impaired concentration.
These chemical and vascular changes also stimulate the autonomic nervous system. The body shifts towards a sympathetic, or ‘fight or flight’, state, increasing heart rate, muscle tension and alertness.
If over-breathing becomes habitual, the body can begin to tolerate lower levels of carbon dioxide as normal. This maintains a state of physiological arousal and can perpetuate a range of symptoms over time, including breathlessness, air hunger, frequent sighing, dizziness, tingling, palpitations, chest tightness, fatigue, poor concentration, headaches, muscle tension, gut motility issues and bloating. These are commonly reported in women with lipoedema and often overlap with autonomic symptoms.
Why This Matters in Lipoedema
Pain in lipoedema is typically explained by changes within the tissue, including microvascular, lymphatic and inflammatory processes. However, breathing pattern disorders may contribute to symptom amplification.
Breathing is closely linked to autonomic function. When it is dysregulated, sympathetic activity increases and parasympathetic regulation is reduced. Pain sensitivity may increase and symptoms may become more widespread in the body.
This is particularly relevant in conditions associated with autonomic dysfunction, including POTS, anxiety-related presentations and gastrointestinal disturbance. Mast cell activation may also contribute to increased sensitivity and symptom reactivity.
For women with lipoedema, this combination may intensify pain and contribute to the persistence of symptoms.
Exercise and Symptom Amplification in Lipoedema
Women with lipoedema frequently report pain, heaviness and a burning sensation during or following relatively low levels of physical activity. This is often described as “lactic acid build-up”. While this is a common interpretation, it does not fully account for the intensity or persistence of symptoms described.
In normal physiology, lactate is produced within muscle during higher-intensity activity when energy demand temporarily exceeds oxygen supply. This is a short-term, local response and is typically experienced as a burning sensation during exertion or shortly afterwards. Under usual conditions, lactate is rapidly cleared and reused by the body, including by the liver (Cori cycle), heart and other skeletal muscle, and does not persist.
Muscle soreness that develops hours to days after exercise is more accurately explained by Delayed Onset Muscle Soreness. This reflects local tissue stress, microscopic muscle fibre disruption and an associated inflammatory response. It is usually characterised by stiffness, tenderness and discomfort on movement, rather than the immediate burning sensation associated with exertion.
These physiological responses are well recognised and generally follow a predictable pattern. However, the symptoms described by many women with lipoedema do not consistently align with these patterns, particularly where discomfort occurs early, is disproportionate to the level of activity, or persists beyond what would be expected.
In some women, a shallow or inefficient breathing pattern may already be present at rest. This reduces physiological reserve and may result in a tendency towards lower carbon dioxide levels even before exertion begins. When activity is introduced, ventilation increases further, and the relative reduction in carbon dioxide may be more pronounced. This lowers the threshold at which symptoms are triggered, meaning that even low levels of exercise may provoke disproportionate discomfort.
During exertion, breathing may increase beyond metabolic demand, particularly where a dysfunctional breathing pattern is present. This can lead to a further reduction in carbon dioxide levels and an amplification of the physiological effects described above, including reduced oxygen delivery, altered tissue perfusion and increased neural sensitivity.
As a result, relatively low levels of exertion may produce symptoms that feel disproportionate to the activity performed.
The Role of Sighing
During periods of stress, anxiety or fatigue, frequent sighing may occur. This is a normal physiological response that transiently increases ventilation and helps reset the breathing pattern.
If frequent sighing becomes habitual, it may contribute to ongoing over-breathing and instability in carbon dioxide levels. It is a sign that diaphragmatic breathing could help your symptoms.
Diaphragmatic Breathing
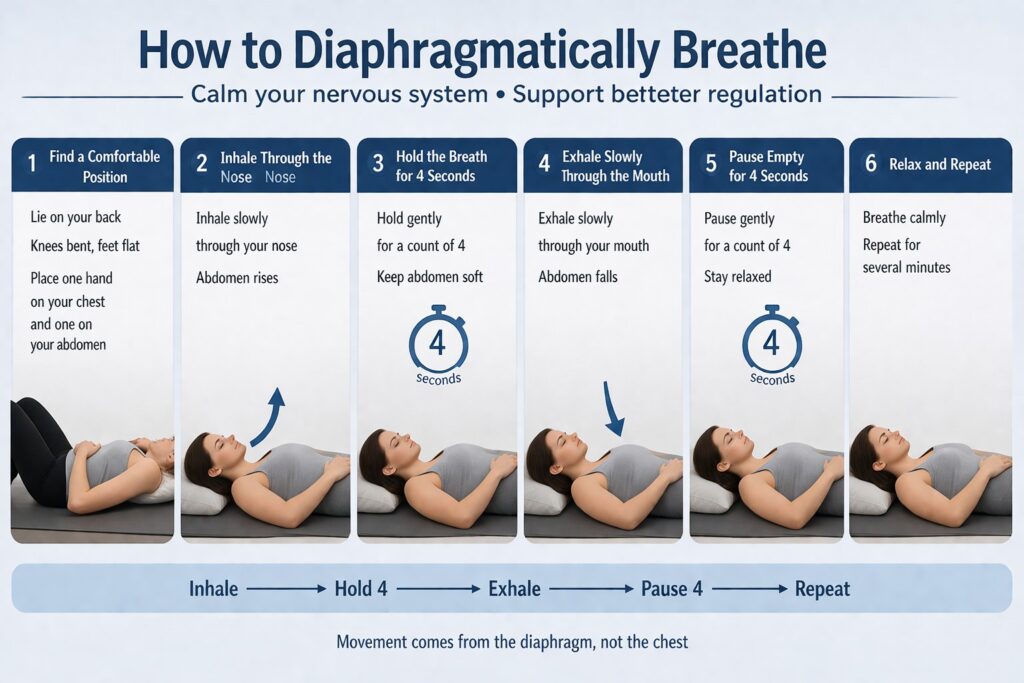
Diaphragmatic breathing is a useful tool to reset breathing. It aims to restore a more efficient pattern.
In normal breathing, the diaphragm performs most of the work, the abdomen rises gently and the upper chest remains relatively still. In breathing pattern disorders, the diaphragm does not move effectively and accessory muscles of the neck (sternocleidomastoid/scalenes) and chest are overused, making breathing more laboured and less efficient.
Diaphragmatic breathing uses slow nasal inhalation with gentle abdominal expansion and minimal upper chest movement, followed by a controlled, prolonged exhalation. Breathing exercises focus on recognising patterns, reducing unnecessary sighing and restoring a steady rhythm through regular practice.
It is likely to feel unfamiliar at first and can take weeks to retrain to properly improve symptoms. Some women notice increased awareness of their breathing, anxiety, a feeling of panic rising or mild discomfort throughout the body as the pattern adjusts.
Supporting Regulation
Managing breathing pattern disorders also involves recognising and reducing triggers such as stress or fatigue, allowing time between activities to release tension, sustaining activity rather than avoiding movement, improving sleep routines and supporting stable blood sugar through regular eating. Relaxation can help reduce background tension and improve overall nervous system regulation.
Summary
Breathing pattern disorders may contribute to pain and systemic symptoms in lipoedema. It is possible that many body systems are also dysregulated in lipoedema. They interact with autonomic dysfunction and may overlap with conditions such as POTS, fibromyalgia and Mast Cell Activation Syndrome. Addressing breathing offers a simple, non-pharmacological approach to support symptom control.