
Introduction
Lipoedema is usually described as a disorder of fat distribution, with disproportionate accumulation of subcutaneous adipose tissue, most commonly in the legs and sometimes the arms. The tissue is often painful, tender and prone to bruising. It has historically been classified by stage and type, according to the distribution and texture of the fat, but those descriptive labels do not explain the full clinical picture.
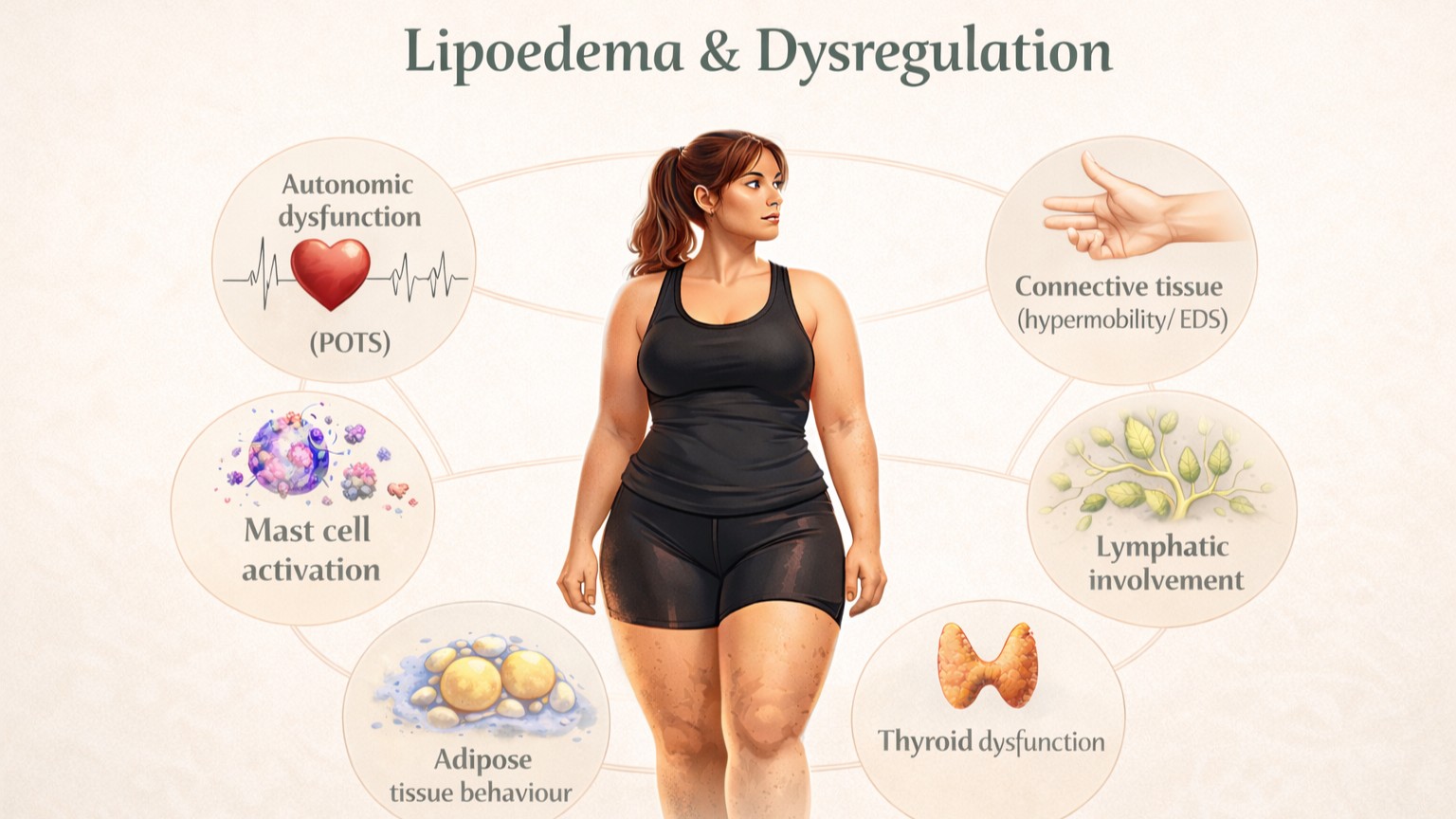
That is where the usual explanation becomes too narrow. In practice, many women with lipoedema do not present only with painful fat, easy bruising and heaviness. They often describe a wider pattern of dysfunction affecting other parts of the body. There may be chronic pain, altered temperature regulation, dizziness, palpitations, food sensitivities, bowel disturbance, abnormal bleeding, pelvic symptoms, hypermobility, poor healing and a general sense that the body has never really behaved in a stable or predictable way.
This matters because lipoedema is not just a matter of where fat is stored. At tissue level, lipoedema reflects dysregulation within the adipose tissue itself: how it is signalled, how it grows, how it responds to hormones and inflammation, and how it resists normal metabolic control. In many patients, that adipose dysregulation appears alongside broader dysregulation across multiple body systems. The fat distribution is obvious, but it is not the whole story of lipoedema and dysregulation.
What Is Regulation?
The body functions through constant co-ordination. Regulation means that systems are communicating properly, responding proportionately and returning to balance after challenge.
Muscles contract and release in the right sequence and with the right tone. They stabilise joints without excessive gripping, they respond to load without overreacting and they allow movement to happen efficiently. Connective tissue provides enough support for structures to hold shape and function, without excessive laxity or collapse.
The autonomic nervous system regulates heart rate, blood pressure, vascular tone and temperature continuously in the background. When a person stands up, blood vessels constrict, circulation adjusts and the body remains stable. When the environment is hot or cold, temperature is controlled within a narrow range.
The vascular system maintains flow and integrity. Capillaries are not excessively fragile, bruising is limited and fluid does not shift unpredictably into tissue.
The immune system also behaves proportionately. It responds when needed and settles again when the stimulus has passed.
The gastrointestinal tract relies on the same principle. Motility, secretion and absorption happen in a coordinated way. Food is tolerated, the bowel moves predictably and the gut does not respond to ordinary intake as if it were a threat.
Hormonal regulation is also dynamic but controlled. Hormones fluctuate across the menstrual cycle, puberty, pregnancy and menopause, but the body accommodates these changes without losing stability.
Regulation, then, is not stillness. It is the ability to adapt without falling out of balance.
What Is Dysregulation?
Dysregulation is the loss of that coordinated control.
The body is still responding, but not in a balanced, proportionate or predictable way. Signals may be amplified, poorly timed, inconsistent or slow to resolve. One system may overreact while another underperforms. Instead of adaptation followed by return to baseline, symptoms persist, fluctuate or appear out of proportion to the trigger.
Muscles may remain tense when they should release, or fail to stabilise when they should support. Joints may move excessively and surrounding tissues are forced to compensate.
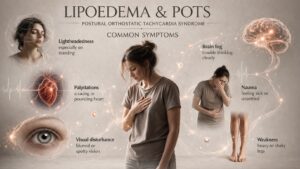
Blood vessels may constrict or dilate inappropriately, leading to colour change, cold extremities, pooling or visible vascular patterning such as livedo reticularis. Autonomic responses may become unreliable, so that standing up produces dizziness, palpitations or tachycardia, known as Postural Orthostatic Tachycardia Syndrome.
Immune signalling may also become exaggerated. Mast cells may release histamine and other mediators too readily, producing flushing, itching, rashes, swelling, food sensitivities or reactions to minor triggers, known as Mast Cell Activation Syndrome. Gastrointestinal function may become irregular, with bloating, constipation, abdominal discomfort or variable food tolerance. Hormonal signalling may lose stability, so symptoms become markedly worse around the cycle or during life stage transitions.
Dysregulation is not one diagnosis. It is a pattern in which several systems are no longer working together in a quiet, efficient and controlled way.
Musculoskeletal & Connective Tissue
Connective tissue provides structural support throughout the body. When that support is altered, joints become less stable and muscles have to work harder to hold the body together. Over time, that constant compensation creates fatigue, chronic pain and recurrent injury.
This helps explain why some patients with lipoedema also describe longstanding tendon problems, hypermobility, bursitis, spinal pathology, sacroiliac pain, disc issues or pain syndromes later labelled as fibromyalgia. The issue is not simply wear and tear. It is that support tissues are not managing load efficiently, and muscles are working continuously to compensate.
There may also be signs of abnormal connective tissue behaviour. Bunions, ganglion cysts and similar changes suggest that connective tissue is not remodelling or responding in a clean, proportionate way. Healing may be slower, scar tissue may behave poorly and minor mechanical issues may progress more than expected. Ehlers Danlos Syndrome may be present
Smooth Muscle & Organ Function
Muscle is not limited to the limbs and spine. Smooth muscle is present throughout the bowel, bladder, blood vessels and uterus, while the heart depends on highly regulated cardiac muscle.
When regulation is lost, these tissues may stop behaving consistently. The bowel may become sluggish or reactive, the bladder may empty poorly or unpredictably and vascular tone may fluctuate. Within the uterus, altered muscular and connective tissue behaviour may contribute to painful periods, heavy bleeding, poor uterine tone or difficulty maintaining pregnancy.
This is important clinically because reproductive symptoms are often treated as separate gynaecological problems, bowel symptoms as gastrointestinal problems and palpitations as cardiac problems. In some women, they are separate. In others, they are different expressions of the same wider loss of control across muscle and connective tissue systems.
Nervous System & Autonomic Control
The autonomic nervous system governs internal stability. When its control becomes unreliable, the body can struggle with posture, circulation, temperature and sensory processing.
That may present as dizziness on standing, palpitations, rapid heart rate, poor exercise tolerance, temperature instability and overwhelming fatigue. The person may feel suddenly unwell simply from standing upright or being in a warm room. The system is reacting, but not regulating smoothly.
Sensory processing may also become amplified. Pressure, light touch, heat, cold or ordinary bodily sensations can feel disproportionate or distressing. This is one reason some patients describe pain that seems too widespread or too severe to be explained by imaging alone. It also helps explain why fibromyalgia is often used as a label in this group. The label may describe the pain state, but it does not explain why that pain state developed.
Sleep disturbance, brain fog, anxiety and low mood also commonly sit within this pattern. That does not mean the symptoms are purely psychological. It means the nervous system is no longer providing steady background regulation, and the emotional and cognitive consequences follow.
This altered regulation also affects how pain is processed. Sensory signalling may become amplified, and the threshold at which stimuli are perceived as painful may be lowered. Pain may persist beyond the point at which tissue injury would normally resolve, reflecting changes in both peripheral and central processing rather than ongoing structural damage.
Vascular & Circulatory System
Lipoedema tissue is commonly associated with easy bruising, heaviness and fluctuation. Those symptoms point towards altered vascular behaviour.
When vascular tone and capillary integrity are less stable, blood vessels may become more fragile and bruising becomes more frequent. Blood may pool in the lower limbs, tissue perfusion may vary and the patient may notice changing colour, temperature or swelling through the day. Some develop Raynaud-type symptoms, others visible mottling such as livedo reticularis.
These are not trivial cosmetic observations. They suggest that circulation is being controlled inconsistently. That contributes directly to pain, heaviness and variability within the tissue.
Lymphatic & Fluid Regulation
The lymphatic system plays a central role in fluid balance, immune surveillance and the clearance of metabolic and inflammatory by-products from tissue.
When this system is functioning effectively, interstitial fluid is collected and returned to the circulation, and inflammatory mediators are cleared in a controlled and efficient way.
In dysregulation, this process may become less effective. Fluid may accumulate within tissue, clearance may be delayed and the local environment may become increasingly congested.
Clinically, this may present as heaviness, a sense of fullness within the tissue, delayed recovery after activity and a tendency towards swelling that fluctuates rather than resolving completely. In some patients, this progresses to a more defined overlap with lymphatic insufficiency.
This is particularly relevant in lipoedema, where the combination of altered vascular behaviour, inflammatory signalling and adipose tissue changes places increased demand on lymphatic function.
Immune Signalling & Tissue Reactivity
Immune dysregulation does not always mean infection or classic autoimmune disease. It can mean that signalling has become exaggerated, poorly controlled or too easily triggered.
Mast cells are part of normal tissue physiology, including within connective tissue and adipose tissue. Their job is to respond to threat and help coordinate inflammatory signalling. When they become overactive or over-responsive, histamine and other mediators may be released too readily. The result can be flushing, itching, hives, swelling, rashes, food sensitivities, alcohol intolerance or reactivity to temperature, stress or minor triggers.
This matters in lipoedema because the tissue is already painful and reactive. Immune signalling that is heightened or poorly resolved may further amplify discomfort, sensitivity and fluctuation. Again, this does not mean every woman with lipoedema has mast cell activation syndrome. It means that dysregulated immune signalling may be part of the wider clinical picture.
Inflammatory Dysregulation
Inflammation is a normal and necessary process. It allows the body to respond to injury, infection and tissue stress. In a controlled state, inflammatory signalling is activated when required and resolves once the stimulus has passed.
In dysregulation, this process does not behave proportionately.
Inflammatory signalling may be persistently activated at a low level, amplified in response to relatively minor triggers, or slow to resolve. This creates an environment in which tissue is continually exposed to inflammatory mediators, even in the absence of clear injury or infection.
Within adipose tissue, this is particularly relevant. Adipose is not passive storage tissue. It is metabolically active and involved in immune signalling. When regulation is lost, inflammatory signalling within adipose tissue may contribute to pain, sensitivity and resistance to normal metabolic processes.
More broadly, inflammatory dysregulation may present in different ways across the body. Some patients describe persistent low-grade pain, fatigue and tissue sensitivity. Others develop more defined inflammatory conditions affecting specific organs or systems.
Within the gastrointestinal tract, this may be reflected in inflammatory bowel conditions such as Crohn’s disease or ulcerative colitis. Within joints and soft tissues, it may contribute to persistent pain states. Within the skin, it may present as rashes, flushing or reactivity.
The common feature is not the specific diagnosis, but the behaviour of the inflammatory response itself. Signalling is no longer tightly controlled, and the body remains in a state of heightened or poorly resolved activation.
This overlaps with immune signalling and mast cell activity, but it is not identical. It reflects a broader issue of how inflammatory processes are initiated, amplified and resolved across multiple tissues.
Autoimmune Expression
Autoimmune conditions represent a further expression of dysregulation within the immune system.
In a regulated state, the immune system is able to distinguish between self and non-self, responding to external threats while maintaining tolerance to the body’s own tissues. This balance is tightly controlled and prevents inappropriate activation.
In dysregulation, this control may be lost. The immune system may begin to recognise self-tissue as a target, leading to sustained inflammatory activity directed against specific organs or systems.
This may become apparent through established autoimmune conditions. In some patients, this includes inflammatory joint disease such as rheumatoid arthritis, where immune activity is directed towards synovial tissue, leading to pain, swelling and progressive joint change. In others, it may affect the thyroid, as seen in autoimmune thyroid disease, altering metabolic control and energy regulation. Within the gastrointestinal tract, inflammatory bowel diseases such as Crohn’s disease or ulcerative colitis reflect immune-driven inflammation of the gut lining.
Connective tissue may also be involved, with autoimmune processes contributing to widespread pain, fatigue and tissue sensitivity. In some cases, patients describe a constellation of symptoms suggestive of immune instability without fitting neatly into a single diagnostic category.
The presence of autoimmune disease is not a feature of lipoedema itself. However, in some patients, it sits alongside other patterns of dysregulation, including altered inflammatory signalling, mast cell activity and tissue reactivity.
What is clinically relevant is not the specific diagnosis alone, but the underlying behaviour of the immune system. When considered alongside other features, autoimmune expression may represent part of a broader pattern of dysregulation affecting multiple systems within the same individual.
Gastrointestinal System
The gastrointestinal system often reflects dysregulation very clearly because it depends on coordinated communication between nerves, muscles, hormones and immune signalling.
When that coordination is lost, the bowel may become slow, sensitive or erratic. Patients may describe constipation, bloating, cramping, abdominal pain, reflux or inconsistent tolerance to food. They may say that a food is tolerated one week and causes a reaction the next.
That pattern is clinically important. It suggests altered signalling rather than a single structural gut disorder. The bowel is often responding as part of a wider dysregulated system rather than as an isolated organ problem.
This may also reflect altered barrier function within the gut. When the integrity of the gut lining is affected, sensitivity to dietary and environmental triggers may increase, further amplifying immune and inflammatory responses.
Endocrine & Hormonal Regulation
Hormones are central to lipoedema. The condition often becomes apparent or worsens at puberty, pregnancy and menopause, which already tells us that adipose tissue is responding to endocrine signalling in an abnormal way.
More broadly, some patients also show evidence of hormonal dysregulation elsewhere. Thyroid dysfunction, polycystic ovary syndrome, major cyclical fluctuation in symptoms and poor tolerance of hormonal transitions may all be part of the picture. The issue is not only that hormones are present, but that tissues are responding to them in an exaggerated, unstable or poorly regulated way.
That is why lipoedema can be understood as dysregulation of adipose tissue itself. The signalling that governs adipose growth, storage, inflammatory behaviour and metabolic responsiveness is not behaving normally.
Hormonal regulation does not occur in isolation. It is closely linked to the nervous system through neuro-endocrine pathways, including the stress response. When this interaction becomes dysregulated, patients may experience exaggerated responses to stress, poor recovery and persistent fatigue, reflecting the combined effect of altered hormonal and neurological signalling.
Metabolic Regulation & Adipose Tissue Behaviour
Adipose tissue is metabolically active and plays a role in energy regulation, hormonal signalling and inflammatory processes.
In a regulated system, adipose tissue responds to metabolic demand in a proportionate way. Fat is stored and mobilised in response to energy balance, and tissue remains responsive to normal regulatory signals.
In dysregulation, this responsiveness is altered. Adipose tissue may become resistant to normal metabolic cues, with fat accumulation occurring in a disproportionate and region-specific way.
This is a defining feature of lipoedema. The issue is not simply excess fat, but altered signalling within adipose tissue itself. Processes that regulate growth, storage, mobilisation and inflammatory behaviour do not function in a predictable or responsive way.
Clinically, this presents as resistance to conventional weight loss approaches, disproportionate fat distribution and persistence of tissue changes despite appropriate lifestyle measures.
Reproductive & Pelvic Health
Reproductive and pelvic symptoms are often significant and should not be reduced to a short list. Many women report painful periods, heavy bleeding, pelvic pain, endometriosis, polycystic ovary syndrome, worsening symptoms around the cycle, miscarriage or difficulty carrying pregnancies to term.
These features matter because they suggest that uterine muscle, connective tissue support, hormonal signalling and inflammatory responses may all be behaving abnormally within the same body. Pelvic symptoms are often treated separately, but when placed alongside vascular instability, hypermobility, pain, bowel disturbance and adipose dysregulation, they form part of a much broader picture.
Generational Patterns
When detailed family histories are taken, patterns often emerge across generations.
The same family may contain different expressions of dysregulation rather than one neat inherited diagnosis. One person may have lipoedema, another hypermobility, another vascular problems, another chronic pain, another bowel disturbance, another miscarriage history or pelvic problems, another autoimmune or inflammatory symptoms. Men may show it too, though not through lipoedema itself.
This generational pattern matters because it suggests inherited vulnerability not simply to one named condition, but to instability in how multiple systems regulate and respond.
What This Means in Lipoedema
Clinically, this changes the frame.
Lipoedema can be understood as dysregulation of adipose tissue: abnormal signalling in how fat is generated, stored, grows, breaks down, behaves and resists normal control. But in many women, that adipose dysregulation does not occur in isolation. It sits within a body that has shown a lifetime of dysregulation, elsewhere in the body as well.
That does not mean every symptom should be collapsed into one diagnosis. Nor does it mean every woman with lipoedema has the same multisystem pattern. It means that clinicians should stop assuming that painful fat explains everything and should stop treating each associated symptom as though it arose independently.
This does not redefine lipoedema as a multisystem disease. It reflects the context in which it presents in clinical practice.
When the wider pattern is recognised, the woman, herself, makes more sense of her symptoms. The history makes more sense. The variability, the poor treatment responses, the repeated dismissals and the accumulation of seemingly unrelated diagnoses begin to fit together.
Conclusion
Lipoedema is not just a pattern of fat distribution. It is a disorder of adipose tissue behaviour and signalling. In many women, that tissue-level dysregulation appears alongside broader dysregulation across connective tissue, muscle, vascular control, immune signalling, gut function, hormonal regulation and reproductive health.
Recognising this does not erase the diagnosis of lipoedema. It sharpens it. It places the condition in a more clinically accurate context and helps explain why so many women present with far more than painful legs and easy bruising.
That is what matters in practice. Not simply naming the fat pattern, but understanding the body in which it exists.