
Introduction
Postural Orthostatic Tachycardia Syndrome (POTS) is a disorder of the autonomic nervous system affecting regulation of circulation during postural change, particularly on transition from lying or sitting to standing.
The nervous system comprises the somatic system, responsible for conscious movement, and the autonomic nervous system, which regulates internal physiological function without conscious input. The autonomic system maintains homeostasis through two integrated branches, sympathetic and parasympathetic, which coordinate heart rate, vascular tone and distribution of blood to maintain arterial pressure and ensure adequate cerebral perfusion. In simple terms, this system keeps blood flow stable without you having to think about it.
POTS reflects failure of autonomic regulation of circulation. The mechanisms that normally stabilise haemodynamics on standing do not function effectively, and circulation is not maintained appropriately in the upright position.
Clinical Presentation
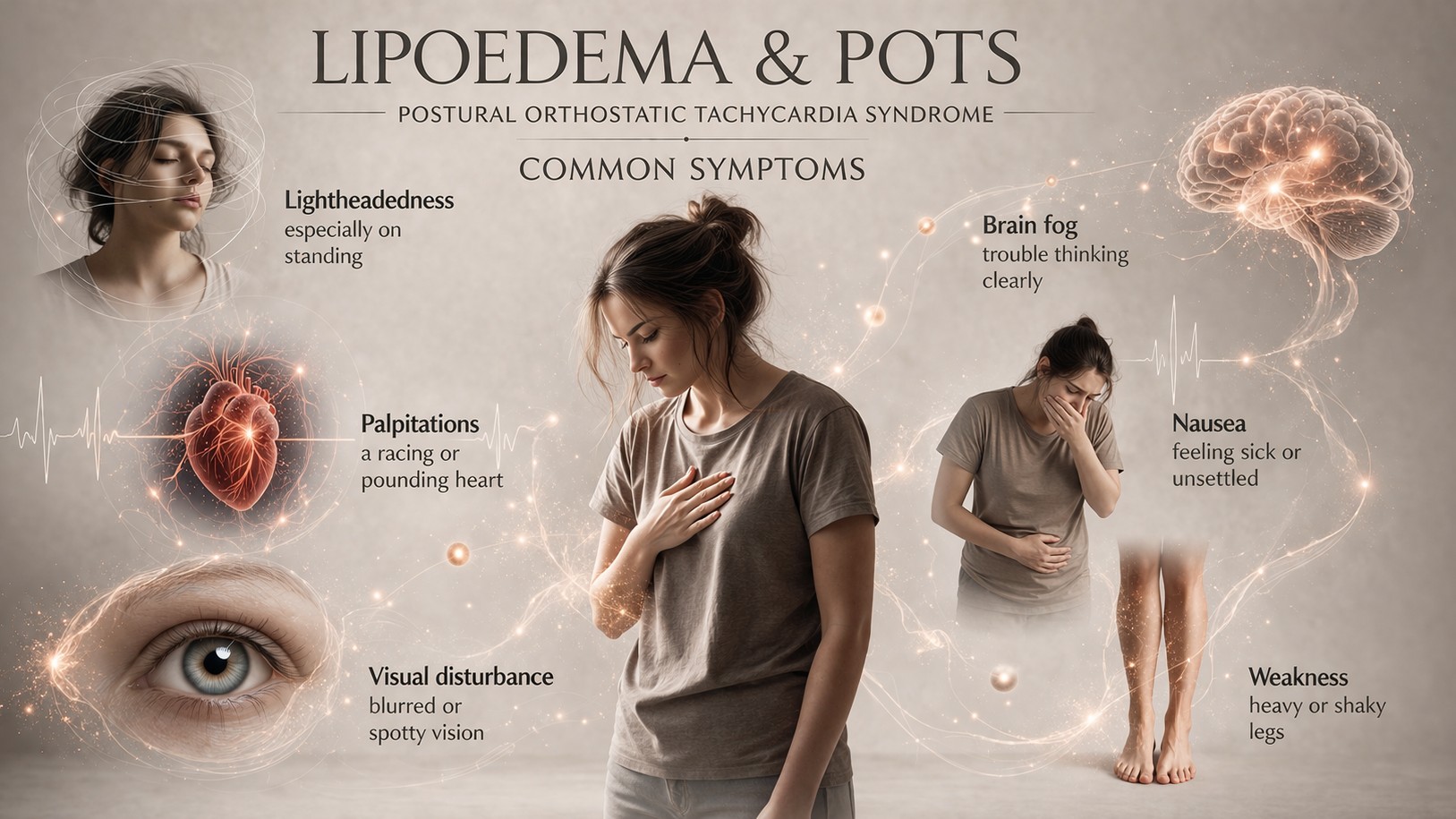
Patients typically describe lightheadedness and presyncope, a sensation of almost fainting, often experienced as dizziness, weakness or a feeling that consciousness may be lost. This reflects reduced blood flow to the brain when upright.
Palpitations correspond to compensatory tachycardia, with the heart beating faster in an attempt to maintain circulation. Some individuals may also experience chest discomfort or shortness of breath, which reflect the strain of this sustained cardiovascular response rather than primary cardiac disease.
Fatigue is frequently disproportionate to exertion and persistent, reflecting the ongoing physiological effort required to maintain circulation. Cognitive impairment, including reduced concentration, slowed processing and what is often described as “brain fog”, occurs as a result of reduced cerebral perfusion.
Visual disturbance, including blurred or tunnel vision, may occur when blood flow to the brain and visual pathways is insufficient. Weakness and a sense of heaviness can develop as blood pools in the lower body.
More widespread autonomic involvement may also be present. Individuals may experience gastrointestinal disturbance, including nausea, altered bowel habit, bloating or abdominal discomfort, reflecting dysregulation of autonomic control within the gut. Sweating and tremor may occur due to heightened sympathetic activity.
Changes in peripheral circulation can also be seen, including colour changes in the hands and feet, which may appear pale, mottled or purple. These reflect altered vascular tone and blood flow in the extremities.
Circulatory Dysfunction in POTS
On standing, gravitational forces cause redistribution of blood into the lower limbs and the splanchnic vasculature, the blood vessels supplying the abdominal organs. This reduces venous return to the heart. In practical terms, less blood is returning to the heart to be pumped around the body.
In normal physiology, this is rapidly corrected through vasoconstriction within the peripheral and splanchnic circulation, alongside a modest increase in heart rate. These adjustments restore venous return, maintain cardiac output and preserve cerebral perfusion. This allows blood flow to the brain to remain stable even when upright.
In POTS, this compensatory response is inadequate. Vascular constriction is insufficient, allowing continued pooling of blood in the lower body. Venous return remains reduced and effective circulating volume is diminished.
The increase in heart rate represents a compensatory response to reduced preload rather than a primary cardiac abnormality. The heart is beating faster to try to maintain circulation, but this does not fully correct the problem. Circulatory stability is not restored and blood flow to the brain remains impaired when upright. Symptoms occur due to the combined effects of impaired circulation and ongoing autonomic activation.
The underlying issue is not pressure itself, but how blood is being distributed and returned to the heart.
Diagnostic Definition
POTS is defined by a sustained increase in heart rate of at least 30 beats per minute within ten minutes of standing in adults, or 40 beats per minute in adolescents aged 12–19 years, in the absence of orthostatic hypotension.
Orthostatic hypotension refers to a drop in blood pressure on standing. In POTS, blood pressure is usually maintained, but heart rate increases excessively.
This physiological response must occur in conjunction with symptoms that are provoked by standing up and relieved by lying down. Diagnosis is based on the relationship between clinical presentation and measurable cardiovascular response to postural change.
Mechanisms Underlying Symptoms
Symptoms arise from failure to maintain effective circulation during upright posture.
Reduced venous return limits cardiac filling and reduces stroke volume. This means less blood is pumped out with each heartbeat. Although heart rate increases, this does not restore normal circulatory efficiency.
Impaired cerebral perfusion produces lightheadedness, visual disturbance and cognitive dysfunction. Persistent pooling within the lower body contributes to heaviness and weakness.
Fatigue reflects the sustained physiological demand required to maintain circulation under conditions of instability. The body is working harder to compensate, even at rest.
Patterns within POTS
POTS represents a diverse pattern of autonomic dysfunction rather than a single disease entity.
Underlying mechanisms may include impaired vasoconstriction, reduced circulating blood volume, increased sympathetic activity or post-viral autonomic disturbance. These describe different ways in which the system regulating circulation can fail.
These mechanisms may coexist and contribute in varying ways to the clinical presentation.
Assessment
Assessment is undertaken to demonstrate how the body responds to postural change.
Tilt table testing allows controlled measurement of heart rate and blood pressure during transition from supine to upright position. This recreates the effect of standing while monitoring how the body responds.
Active stand testing may also be used.
The defining feature is a sustained increase in heart rate without a corresponding fall in blood pressure.
What POTS is not
POTS is not a structural cardiac disorder and does not arise from primary pathology of the heart.
It is not defined by symptoms alone. Although symptoms may overlap with anxiety, the condition reflects dysfunction of autonomic regulation rather than a primary psychological disorder.
POTS & Lipoedema
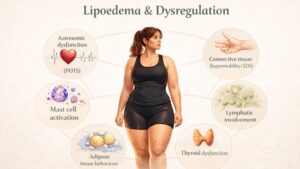
POTS represents dysregulation of autonomic control of circulation. Lipoedema is a disorder of subcutaneous tissue, but this tissue exists within a vascular and neurovascular environment.
Altered microvascular function, increased capillary fragility and disordered fluid distribution are recognised features of lipoedema. These changes affect how fluid and blood behave within the tissue, but they do not in themselves define autonomic dysfunction.
Where vascular tone is reduced, gravitational pooling of blood is more likely to occur on standing. This reduces venous return and necessitates compensatory increases in heart rate. This provides a physiological basis for overlap.
Symptoms including lightheadedness, fatigue, heaviness and pain may therefore occur in both conditions. These reflect shared mechanisms of vascular and circulatory dysregulation rather than a shared diagnosis.
Current evidence does not demonstrate that POTS is a defining feature of lipoedema, nor that lipoedema causes POTS. Where both conditions are present, symptoms may be amplified through combined effects on systemic circulation and tissue behaviour.
Conclusion
POTS is a disorder of autonomic regulation in which haemodynamic stability is not maintained during postural change.
Symptoms arise from impaired cerebral perfusion and compensatory tachycardia. In practical terms, the body is unable to maintain stable circulation when upright.
Although distinct conditions, POTS and lipoedema may intersect through shared physiological mechanisms involving vascular control and fluid distribution. Recognising this overlap without conflating the conditions allows for accurate interpretation and appropriate clinical management.
Bibliography
Freeman R, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and postural tachycardia syndrome. Clinical Autonomic Research. 2011;21(2):69–72.
Raj SR. Postural tachycardia syndrome (POTS). Circulation. 2013;127(23):2336–2342.
Arnold AC, Ng J, Raj SR. Postural tachycardia syndrome: diagnosis, physiology, and prognosis. Autonomic Neuroscience. 2018;215:3–11.
Vernino S, Bourne et al. Postural Orthostatic Tachycardia Syndrome (POTS): state of the science and clinical care. Autonomic Neuroscience. 2021;235:102828.
Michelini S, Morrone A, Di Renzo L, De Lorenzo A. Lipedema: diagnostic and management challenges. International Journal of Molecular Sciences. 2022;23(12):6621.